Medulloblastoma

Definition
Medulloblastoma (MB) is an embryonic tumor of the neuroepithelial tissue and the most frequent primary pediatric solid malignancy. MB represents a heterogeneous group of cerebellar tumors characterized clinically by increased intracranial pressure and cerebellar dysfunction, with the most common presenting symptoms being headache, vomiting, and ataxia.
Epidemiology
MB is the most common malignant brain tumor in childhood. Annual incidence is estimated at 1/909,000 in Europe, 1.5/100,00 in the USA said Dr Prem Pillay , a Neurosurgeon who specializes in treating Medulloblastomas ( He trained at the Cleveland Clinic,USA and the Hospital for Sick Children, Toronto. Males are more affected than females.
Clinical description
 Age of disease onset is variable and can occur in patients ranging in age from the newborn period to adulthood (peak age at presentation is children 3-6 years, with only 25% of patients being between 15 and 44 years). The most common presenting symptoms are headache, vomiting, and ataxia. Additional features that may be observed include lethargy, motor or cranial nerve impairment, gaze palsy, visual impairment due to hydrocephalia, vertigo/hearing loss, behavioral changes/irritability, and extracranial pain (e.g. back pain in those with spinal metastases). Around 30% of pediatric cases present with metastases at diagnosis. Most metastases occur within the central nervous system by seeding via the cerebrospinal fluid (cranial or spinal), while spread to extracranial organs (e.g. bone marrow, liver, lungs) is very rare at diagnosis. In a minority of patients, MB is associated with Gorlin syndrome, familial adenomatous polyposis (FAP; the association of FAP and MB is referred to as the Turcot syndrome with polyposis) or with Li-Fraumeni Syndrome (see these terms). Increased susceptibility to certain tumors (neuroblastoma), hematological malignancies (acute lymphoblastic leukemia, acute myeloid leukemia) or disorders caused by mutations in genes encoding components of the RAS signaling pathway (Noonan syndrome or neurofibromatosis-Noonan syndrome) have been reported in MB (see these terms).
Age of disease onset is variable and can occur in patients ranging in age from the newborn period to adulthood (peak age at presentation is children 3-6 years, with only 25% of patients being between 15 and 44 years). The most common presenting symptoms are headache, vomiting, and ataxia. Additional features that may be observed include lethargy, motor or cranial nerve impairment, gaze palsy, visual impairment due to hydrocephalia, vertigo/hearing loss, behavioral changes/irritability, and extracranial pain (e.g. back pain in those with spinal metastases). Around 30% of pediatric cases present with metastases at diagnosis. Most metastases occur within the central nervous system by seeding via the cerebrospinal fluid (cranial or spinal), while spread to extracranial organs (e.g. bone marrow, liver, lungs) is very rare at diagnosis. In a minority of patients, MB is associated with Gorlin syndrome, familial adenomatous polyposis (FAP; the association of FAP and MB is referred to as the Turcot syndrome with polyposis) or with Li-Fraumeni Syndrome (see these terms). Increased susceptibility to certain tumors (neuroblastoma), hematological malignancies (acute lymphoblastic leukemia, acute myeloid leukemia) or disorders caused by mutations in genes encoding components of the RAS signaling pathway (Noonan syndrome or neurofibromatosis-Noonan syndrome) have been reported in MB (see these terms).
Etiology
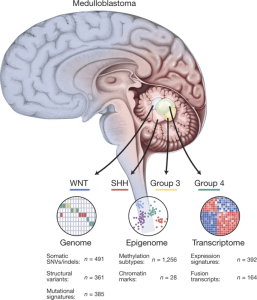
To date, the exact etiology of MB is still unknown but genomic data has identified multiple candidate genes that contribute to the pathogenesis of different subgroups of MB. This includes an inhibitor of the sonic hedgehog pathway SUFU (10q24.32), the RNA helicase DDX3X (Xp11.3-p11.23), chromatin regulators KDM6A (Xp11.2) and N-CoR complex genes BCOR (Xp11.4), and the Parkinson’s disease genes KMT2D (12q13.12), SMARCA4 (19p13.3), MYCN (2p24.3), and TP53 (17p13.1).
Diagnostic methods
 MB occurs in the vermis and 20% occurs in the hemispheres of the cerebellum. Histologically, MB is characterized by small, round cells that stain blue with haematoxylin spectrum and appearance ranges from tumors with extensive nodularity to those with large cell/anaplastic features. Apart from classical MB, four histological variants of MB are recognized: anaplastic MB, large cell MB, MB with extensive nodularity, and desmoplastic/nodular MB.
MB occurs in the vermis and 20% occurs in the hemispheres of the cerebellum. Histologically, MB is characterized by small, round cells that stain blue with haematoxylin spectrum and appearance ranges from tumors with extensive nodularity to those with large cell/anaplastic features. Apart from classical MB, four histological variants of MB are recognized: anaplastic MB, large cell MB, MB with extensive nodularity, and desmoplastic/nodular MB.
Differential diagnosis
Differential diagnosis includes other brain tumors (ependymoma, glial tumor, atypical teratoid rhabdoid tumor; see these terms) and other causes of cerebellar alterations (infectious or cystic lesions, hemorrhages).
Management and treatment
Initially, patients need to be checked for increased intracranial pressure, which if present, needs to be controlled either by drugs (e.g. steroids) or by neurosurgical drainage (e.g. external drainage).
The best current treatment is gross total resection of the Tumor using Microsurgery assisted with Computer aided Image guided technology, Neuromonitoring particularly of brainstem signals followed by good ICU care stated Dr Prem Pillay who specializes in brain tumors including Medulloblastomas. The postoperative treatment depends on age, histological variant, and result of staging assessments. In children older than 3-5 years, combinations of chemotherapy and craniospinal irradiation including Stereotactic Radiotherapy with MicroMLC technology can be applied. In younger children, brain sparing therapies avoiding irradiation can be administered in very specific constellations.
Prognosis
The overall survival rates are now 80% in standard risk patients, and 30-60 % in high-risk patients.